Limb Loss
It is estimated that 1.7 million people in the US have undergone an amputation. 185,000 Americans undergo amputations each year, 97% of which are lower limb. The most common cause in the US for an amputation is diabetes, and 1 out of 185 people diagnosed with diabetes will suffer a limb loss.* Traumatic loss of limb takes its toll as well: between 2001 and 2010, 816 Americans had lost a limb while performing military service in Iraq or Afghanistan.** In countries plagued by landmines from past and current conflicts, as many as 95% of the amputations in a given country may be traumatic,*** and it is estimated that 0.5% of the world population is in need of a prosthetic or orthotic device.
Prosthetic devices can vary widely in functionality, from prostheses that provide basic support for walking for a lower limb amputee or non-functional devices that look like an upper limb amputee’s hand to prostheses that have motorized, articulated joints controlled by electromyographic (“EMG”) sensors placed on the skin over the muscles on the residual portion of the limb where they record the muscle activity. EMG signals are interpreted by the prosthetic limb’s electronic controller, and the intended movement the EMG profile signals is then performed by the prosthetic limb. Such state-of-the-art devices have improved vastly in the last decade in mimicking natural human movements, allowing users to be better able to navigate rough terrain, climb stairs or grasp objects.
One of the challenges with EMG-controlled prosthetic devices, however, is that, depending on its placement, a sensor on the skin may be picking up signals from more than one muscle at a time, which can degrade the performance of the prosthesis and frustrate its user.
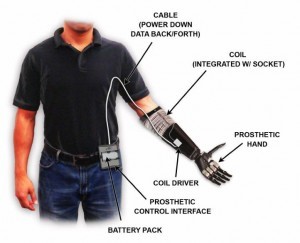
Fully implantable sensors can be placed very specifically in the muscles needed for prosthesis control from which they could give clear and repeatable EMG data to the prosthesis controller, allowing for much more intuitive control of a device. AMF has taken on the challenge of developing such an implant, which we call the Implantable MyoElectric Sensor, or IMES. Packaged in a similar way to the microstimulator, it is a matchstick-sized device which can be implanted into the target muscles through a small incision. The EMG signals are transmitted wirelessly via a radio-frequency coil worn over the implant site from the muscles to the prosthesis controller, which interprets the signals and sends a command to the prosthesis to perform the intended movement.
CAUTION: Investigational device. Limited by Federal (OR USA) law to investigational use.
*LLIC and the Limb Loss Research and Statistics Program (LLR&SP) Fact Sheet Revised 2007
**Congressional Research Service Report “U.S. Military Casualty Statistics: Operation New Dawn, Operation Iraqi Freedom, and Operation Enduring Freedom” September 28, 2010
***Range of Motion Project, 2008
+International Committee of the Red Cross Physical Rehabilitation Programmes 2009 Report